Gait Symmetry Restoration in Patients with Common Neurological Diseases During a Body-Weight Supported Treadmill Therapy Program-A Case Series Study
Eldar Vinarov*
Department of Physiotherapist, Physiotherapist at Cerebrum clinic, Tashkent, Uzbekistan
- Corresponding Author:
- Eldar Vinarov
Department of Physiotherapist,
Physiotherapist at Cerebrum clinic, Tashkent,
Uzbekistan,
E-mail: eldar.vinarov@gmail.com
Received date: October 16, 2023, Manuscript No. IPMCRS-23-18009; Editor assigned date: October 19, 2023, PreQC No. IPMCRS-23-18009 (PQ); Reviewed date: November 02, 2023, QC No. IPMCRS-23-18009; Revised date: November 09, 2023, Manuscript No. IPMCRS-23-18009 (R); Published date: November 16, 2023, DOI: 10.36648/2471-8041.9.10.328
Citation: Vinarov E (2023) Gait Symmetry Restoration in Patients with Common Neurological Diseases during a Body-Weight Supported Treadmill Therapy Program-A Case Series Study. Med Case Rep Vol.9 No.10: 328.
Abstract
Background: Gait disorders accompanied by significant between-limb asymmetry are common in neurological patients and increase the risk of accidental falls and physical disability. If the asymmetry is not sufficiently reduced early in the rehabilitation process, the impact of compensatory mechanisms may lead to its worsening and subsequent difficult and ineffective treatment in the later phase of rehabilitation.
Methods: Four patients with various neurological conditions (neuromuscular disease, post-stroke paresis, radicular syndrome and PNS injury) completed a treatment program combining ten sessions of body-weight supported treadmill therapy and conventional physiotherapy. Gait parameters and symmetry indexes were measured and evaluated at the baseline, during every other session and their development was mutually compared.
Results: After ten sessions, the patient with radicular syndrome had an almost symmetrical gait across all monitored parameters. Similarly, almost complete gait symmetry restoration was observed in a patient with neuromuscular disease. Slight gait asymmetry persisted in the post-stroke patient, but within the acceptable range for all gait parameters. The patient after the PNS injury showed an asymmetry outside the acceptable range, but only in the swing time and the swing/stance time ratio.
Conclusions: The study confirmed the potential of bodyweight supported treadmill therapy in restoring gait symmetry in patients with various neurological conditions. This treatment approach holds the promise of effective gait retraining regardless of the origin and nature of the neurological impairment.
Keywords
R-Force; Antigravity treadmill; Post-stroke paresis; Neuromuscular disease; PNS injury; Radicular syndrome; Symmetry index; Gait parameters
Introduction
Neurological disorders constitute 12% of total deaths globally, 6.3% of the global burden of disease and contribute to 92 million disability-adjusted life years [1]. The patient perceives the loss or reduction of mobility as the biggest limitation in their daily activities [2]. Gait impairment is a common disability in neurological patients, increasing their risk of falling and loss of independence in daily activities [3]. Various neurological conditions are accompanied by specific gait pathologies - weakness, spasticity, loss of proprioception and coordination, pain and other impairments can contribute to the disturbance of the patient's walking [2]. If during walking differences in the bilateral behavior of the lower extremities occur, gait symmetry has been disturbed, causing decreased gait velocity, balance and bone mineral density in the paretic limb and increased metabolic cost. Thus, the main goal of rehabilitation care should be to design an appropriate treatment plan that will lead to partial or complete restoration of gait symmetry [4]. If the asymmetry is not sufficiently reduced early in the rehabilitation process, the impact of compensatory mechanisms may lead to its worsening and subsequent difficult and ineffective treatment in the later phase of rehabilitation [5].
Due to the different nature of individual neurological disorders and the origin and manifestation of their gait asymmetry, the use of a uniform rehabilitation approach can be challenging. For some indications, pharmacological treatment and deep brain stimulation are used to improve walking kinematics, but they have not shown a positive effect on walking asymmetry [4]. In patients who develop a pathological gait accompanied by asymmetry due to compression of the spinal root in the intervertebral space, invasive surgery can contribute to the restoration of gait symmetry [6]. Similarly, most Peripheral Nervous System (PNS) and Central Nervous System (CNS) injuries are accompanied by surgery and subsequent rehabilitation care [7]. A properly designed exercise and walking protocol has proven effective in restoring symmetry in patients with Parkinson's disease and in patients recovering from stroke and spinal cord injury [8-11]. Clinical evidence evaluating gait symmetry and its restoration during the rehabilitation of neurological patients is insufficient and practically non-existent for most indications. Nevertheless, it can be assumed that with a properly designed gait retraining protocol, it is possible to achieve positive changes in walking symmetry across various neurological indications.
The main obstacle in incorporating walking training into the treatment program of neurological patients in the early rehabilitation phase is their impaired balance and subsequent increased risk of falling. The muscles are usually weak and unable to withstand the patient's entire body weight. Body- Weight Supported Treadmill Therapy (BWSTT) is practically the only option for these patients to start gait retraining. This approach allows the provision of full or partial body-weight support to the patient, thus preventing the risk of overloading and falling. Body weight support reduces the need for compensation in the case of painful conditions (e.g. radicular syndromes or PNS injury) and thus accelerates the restoration of walking symmetry. The positive effect of BWSTT has already been demonstrated in neurological patients with various indications, in post-stroke survivors, patients with Parkinson's disease, cerebral palsy and those after spinal cord injury [12-20]. The benefit in the restoration of walking symmetry was demonstrated only in post-stroke patients [9,10].
The aim of this case series study is to demonstrate and mutually compare the impact of BWSTT in patients with different neurological conditions on symmetry restoration of various gait parameters - stance time, step length, step time, swing time, swing/stance time ratio and weight bearing proportion. Due to its scope, the research does not aim to draw general conclusions, but rather to explore the possibilities of BWSTT in a neurological population.
Materials and Methods
Patients recovering from a neurological disorder as part of a routine treatment program provided in a rehabilitation facility underwent 10 sessions of BWSTT followed by conventional physiotherapy. The main condition for admission was a gait asymmetry exceeding 10% in terms of the calculated symmetry index for at least 3 examined gait parameters and a unique neurological indication within the treated patient group. Patients were subsequently assessed for BWSTT eligibility and those found to have contraindications - severe cardiovascular disease, bronchial asthma, angina pectoris, disc herniation, pregnancy, epilepsy, or any conditions with increased abdominal pressure - were excluded from the study. The study design followed the 1975 Declaration of Helsinki ethical guidelines adopted by the Convention on Human Rights and Biomedicine of the Council of Europe (1997) and by the General Assembly of the World Medical Association (1997-2000) [21]. Before starting the treatment program, all participants were informed about its course and possible results publication and confirmed their interest by signing an informed consent.
The therapy was performed with BWSTT technology operating on the principle of positive pressure (BTL Industries Ltd.). The patient's weight is completely or partially "lightened" during the therapy, enabling gait retraining without the risk of excessive load on the lower limbs. Before starting the exercise, the patient is integrated into an inflatable bag surrounding the treadmill by means of a zipper located in the shorts he has already put on. The system is then calibrated to the patient's weight and the bag is inflated with positive pressure. The lower half of the patient's body is part of the inflated bag, which prevents falls and injuries. The operator can change treadmill inclination in the range of 0-15%, speed in the range of -8 km/h to 25 km/h and bodyweight support in the range of 0-100% before and during each therapy. It is assumed that the patient will notice at least minimal progress in the set parameters during the treatment program.
Gait parameters - stance time, step length, step time, swing time and weight loading proportion - were automatically recorded at the baseline screening and during every other session for both limbs using load cells integrated within the treadmill. For the purpose of evaluating the reduction of gait asymmetry, the swing/stance time ratio was added to these parameters and the Symmetry Index (SI) was calculated for all obtained values using the formula [22]:
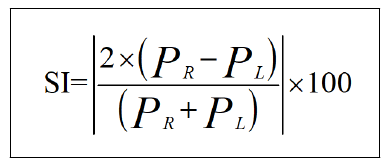
PR refers to the value of the gait parameter measured on the right limb or, in patients who have a clearly defined affected side, on the affected limb. Similarly, PL corresponds to the gait parameter value measured on the left or unaffected limb. For the purpose of evaluating gait asymmetry, the SI level of 10%was chosen as the limit-gait parameters reaching an SI value below this level were evaluated as acceptable, while parameters exceeding this value were evaluated as unacceptable. An SI value equal to 0% corresponds to complete symmetry and a value of 100% to total asymmetry.
Data processing and graphical evaluation was performed in a custom-written script (MatLab R2010b, Mathworks, Inc., Narick, MA, USA).
Results
Four patients with different neurological conditions were recruited and completed the entire treatment program. Positive progress was noted in all of them in terms of acceptance of therapy and reduction of asymmetry. Patients' demographics and indications are summarized in Table 1.
| Neuromuscular disease | Post-stroke paresis | Radicular syndrome | PNS injury | ||
|---|---|---|---|---|---|
| Gender | M | W | W | M | |
| Age | 32 | 69 | 41 | 39 | |
| Affected limb | NA | R | L | L | |
| Speed (km/h) | Initial value | 1.8 | 1.8 | 1 | 2 |
| Final value | 2 | 1.8 | 1.5 | 3 | |
| Inclination (level) | Initial value | 0 | 1 | 0 | 0 |
| Final value | 0 | 2 | 0.5 | 1 | |
| Weight support (%) | Initial value | 50 | 50 | 50 | 50 |
| Final value | 50 | 21 | 12 | 50 | |
Table 1: Patients’ demographics.
During the baseline BWSTT, patients reported a comparable degree of asymmetry across measured parameters. While the post-stroke patient showed the greatest asymmetry, the patient with radicular syndrome recorded the smallest asymmetry. The patient with the smallest degree of pre-asymmetry also experienced the greatest improvement. After ten sessions, the patient with radicular syndrome had an almost symmetrical gait across all monitored parameters. Similarly, almost complete gait symmetry restoration was observed in a patient with neuromuscular disease after the end of the study course. Slight gait asymmetry persisted in the post-stroke patient, but within the acceptable range for all gait parameters. The patient after the PNS injury showed an asymmetry outside the acceptable range, but only in the swing time and therefore also the swing/ stance time ratio.
Stance time
Unacceptable stance time asymmetry recorded during the baseline BWSTT screening in all patients reached below the level of unacceptability in the course of subsequent sessions, down to the level of 4% SI for all indications. Due to the resulting SI value of around 1% in patients with radicular syndrome and neuromuscular disease, almost complete symmetry restoration can be stated. Interestingly, while in the post-stroke patient and the patient after PNS injury the stance time value was higher in the affected limb, in the patient with radicular syndrome it was in favor of the unaffected limb. During individual sessions, there was a gradual decrease in the symmetry index across all indications. Only in the patient with neuromuscular disease was the somewhat dynamic development accompanied by two value fluctuations between the fourth and eighth session (Figure 1).

Figure 1: Horizontal bar graphs allow you to monitor the detailed development of the between-limb difference for individual indications. The lower curves of the symmetry index offer a mutual comparison of asymmetry development during individual sessions.
Step length
The step length parameter reached an unacceptable level only in patients after PNS injury and neuromuscular disease. For the other two indications, the pre-value was within the limits of acceptability. The patient with radicular syndrome achieved full symmetry restoration after only 3 sessions, the other patients reached below 6% SI asymmetry after 10 therapies. In all patients with a unilateral disorder, the unaffected limb made a longer step length than the affected limb. The largest absolute decrease in the symmetry index during the therapy course was experienced by a patient with a neuromuscular disease (Figure 2).

Figure 2: A comparison of the development of gait parameters for individual indications is shown on horizontal bar graphs. The detailed progression of gait symmetry is visualized by the lower curve graph.
Step time
All but one patient showed a step time asymmetry exceeding the SI level of 20% during the baseline screening. In a patient suffering from radicular syndrome, an acceptable SI value of 6% was measured, which was reduced to only 0.5% during 10 sessions, indicating almost complete symmetry restoration. Neuromuscular and PNS injury patients reached an acceptable degree of asymmetry through therapy, namely 7.5% and 4.9%, respectively. The post-stroke patient remained the only patient who, despite a significant decrease, did not fall below the 10% level of acceptability. Similar to stance time, the patient with radicular syndrome showed the opposite trend between affected and unaffected limb than post-stroke and PNS injury patients. For those, a longer step time was measured on the unaffected limb, whereas the radicular syndrome patient spent a longer step time on the affected limb (Figure 3).

Figure 3: The top four graphs are used to display the development of the step time parameter for both limbs in individual patients. The development of the symmetry index during the treatment course is shown in the lower curve graph.
Swing time
From the point of view of swing time, the degree of gait asymmetry during the baseline screening reached an unacceptable level in all patients, by more than 22%. The largest asymmetry, almost 50%, was shown by the post-stroke patient, who, surprisingly, gained almost complete symmetry restoration during the BWSTT program. Neuromuscular disease and radicular syndrome patient got below 4% asymmetry with gait retraining, PNS injury patient did see a significant decrease, but did not reach the 10% level of acceptability. While in PNS injury and post-stroke patients a longer swing time was measured for the unaffected limb, the trend was opposite in the radicular syndrome patient (Figure 4).

Figure 4: Comparison of swing time between both limbs across individual indications is offered by the top four horizontal bar graphs. The resulting symmetry index of the same parameter and its development during the treatment program is shown on the lower curve graph.
Swing/Stance time ratio
Baseline Swing/Stance time ratio recorded the largest between-limb difference in the post-stroke patient. Also, patients with neuromuscular disease and radicular syndrome showed a significant asymmetry exceeding 90%. All of these participants reached below 4% swing/stance time SI after 10 sessions, despite large baseline asymmetry. Asymmetry in a patient after a PNS injury was reduced from 56.8% to 16.4% during the treatment program and was the only one that did not reach the level of acceptability (Figure 5).

Figure 5: The swing/stance time ratio for both limbs for individual indications is visualized on horizontal bar graphs, while the development of gait symmetry is expressed through the symmetry index on the lower curve graph.
Weight-bearing proportion
Two of the four patients experienced complete symmetry restoration in terms of weight bearing proportion during the gait retraining program-both the patient with neuromuscular disease and the radicular syndrome patient. The post-stroke patient went from the initial 20% asymmetry to below 2% and reported the greatest absolute decrease. The patient after a PNS injury did not notice any change in absolute value of gait asymmetry-the value of the symmetry index fluctuated during the study course, but eventually reached the initial 4% level. Interestingly, greater weight bearing gradually shifted from the unaffected limb to the affected limb. In the other patients, this transformation was not so pronounced; the weight was mainly borne by the unaffected limb (Figure 6).

Figure 6: The ratio of weight load for both limbs and its development during the treatment program for individual indications is visualized on horizontal bar graphs, while a comparison of the development of walking symmetry is shown on the bottom curve graph.
Discussion
The current case series study outlined the potential of BWSTT in restoring gait symmetry in patients with various neurological conditions. Despite the different nature of the disability in the individual indications, remarkable progress was observed in all patients. This is a very promising finding not only from the point of view of postoperative care, but also from the point of view of long-term neurological rehabilitation. Improving gait parameters and their asymmetry can bring patients the desired independence in daily activities without fear of falling, overloading or injury. The extent of improvement during a treatment program consisting of only 10 sessions can also be positively perceived. Two of the four patients achieved almost complete restoration of symmetry across all monitored gait parameters. Three-quarters of the patients fell below the acceptable limit of asymmetry in all parameters, and only one patient preserved asymmetry exceeding this limit, but only in the swing time and swing/stance time ratio parameters. This rapid improvement suggests enormous potential in the treatment and research of BWSTT.
To explain the effect of BWSTT in restoring symmetry in patients with various neurological conditions, it is necessary to outline the principle of the therapy itself, but also the origin of the gait asymmetry of the given condition. The most significant improvement was noted in patients with radicular syndrome and neuromuscular disease. In radicular syndrome, radiating pain during walking is considered to be the main cause of gait pathology and asymmetry, while in neuromuscular disease, the source of the between-limb difference is primarily muscle weakness [23,24]. Both symptoms make walking uncomfortable or impossible, not only during everyday life, but also during a routine overground gait retraining program. Partial or full bodyweight support during gait retraining enables adaptation to the correct walking cycle in the first weeks of rehabilitation without the risk of overloading weakened muscles, but also without the need for compensatory activities due to pain. The patient is thus able to practice the correct gait pattern and, with gradually decreasing body-weight support, also to the load of his own weight.
A similar principle works for post-stroke patients to facilitate their neuromotor recovery. BWSTT therapy is commonly used as a task-specific intervention inducing gait recovery with a restored symmetrical pattern [25]. In addition, the system reduces the risk of falling, which is quite high in patients with impaired balance, who are mostly of an older age, as is the case with the post-stroke patient in the present research. PNS injury recovery is the most complex in terms of healing and gait restoration. It depends on the severity of the impairment and the extent of the necessary reinnervation, but satisfactory functional recovery is not always possible [26]. This may explain the findings of the present study, in which a patient recovering from a PNS injury, as the only preserved asymmetry of an unacceptable extent.
The scope and focus of the research is not intended to prove the effectiveness of BWSTT for various neurological indications, but only to outline the potential of this advanced technology in the treatment of neurological patients. A larger sample size, ideally supplemented by a control group allowing mutual results comparison, would be required to evaluate BWSTT effectiveness. Future trials could also focus on comparing the improvement of asymmetry and gait impairment between cohorts of patients with different neurological diseases. It could bring a new perspective on the functional recovery of patients after conditions affecting the CNS or PNS.
Conclusion
The current study presents a unique research comparing the effect of body-weight supported treadmill therapy on the detailed development of gait symmetry in neurological patients. A positive effect on walking parameters and their between-limb symmetry was confirmed in all patients, regardless of the nature of their neurological disability. Ten exercise sessions enabled almost complete gait symmetry restoration in patients with radicular syndrome and neuromuscular disease. Slight gait asymmetry persisted in the post-stroke patient and the patient after peripheral nervous system, but in both patients an improvement was noted across all monitored gait parameters.
Although the present study represents only small-scale research, the results confirmed the potential of body-weight supported treadmill therapy in restoring gait symmetry in patients with various neurological conditions. The principle and operation of this treatment approach holds the promise of effective gait retraining regardless of the origin and nature of the neurological impairment.
References
- (2006) Neurological disorders: Public health challenges. World Health Organization.
- Pearson OR, Busse ME, van Deursen RWM, Wiles CM (2004) Quantification of walking mobility in neurological disorders. QJM 97: 463–475.
[Crossref], [Google Scholar], [Indexed]
- Moon Y, Sung JH, An R, Hernandez ME, Sosnoff JJ (2016) Gait variability in people with neurological disorders: A systematic review and meta-analysis. Hum Mov Sci 47: 197-208.
[Crossref], [Google Scholar], [Indexed]
- Meder KG, LoJacono CT, Rhea CK (2022) A systematic review of non-pharmacological interventions to improve gait asymmetries in neurological populations. Symmetry 14: 281.
[Crossref], [Google Scholar]
- Buckley C, Micó-Amigo ME, Dunne-Willows M, Godfrey A, Hickey A, et al. (2020) Gait asymmetry post-stroke: Determining valid and reliable methods using a single accelerometer located on the trunk. Sensors 20:37.
[Crossref], [Google Scholar], [Indexed]
- Wang J, Zou Q, Li S, Tang R, Yang X, et al. (2022) Gait asymmetry of lower extremities reduced immediately after minimally invasive surgery among patients with lumbar disc herniation. Clin Biomech 98: 105720.
[Crossref], [Google Scholar], [Indexed]
- Lopes B, Sousa P, Alvites R, Branquinho M, Sousa AC, et al. (2022) Peripheral nerve injury treatments and advances: One health perspective. Int J Mol Sci 23: 918.
[Crossref], [Google Scholar], [Indexed]
- Hubble RP, Naughton G, Silburn PA, Cole MH (2018) Trunk exercises improve gait symmetry in Parkinson disease. Am J Phys Med Rehabil 97: 151–159.
[Crossref], [Google Scholar], [Indexed]
- Hassid E, Rose D, Commisarow J, Guttry M, Dobkin BH (1997) Improved gait symmetry in hemiparetic stroke patients induced during body weight-supported treadmill stepping. J Neuro Rehab 11: 21-26.
- Combs SA, Dugan EL, Ozimek EN, Curtis AB (2013) Bilateral coordination and gait symmetry after body-weight supported treadmill training for persons with chronic stroke. Clin Biomech 28: 448-453.
[Crossref], [Google Scholar], [Indexed]
- Machado LL, Lucas K, Behrman AL (2023) Activity-based restorative therapy promotes progression from asymmetry to symmetry in posture and gait in a child with chronic, incomplete spinal cord injury. Children 10: 594.
[Crossref], [Google Scholar], [Indexed]
- Prunerová A, Vinarov E (2023) Increase in metabolic rate and related parameters during an antigravity treadmill exercise program in neurological patients. J Neurodegenero Dis Disord 6: 4.
- Duncan PW, Sullivan KJ, Behrman AL, Azen SP, Nadeau SE, et al. (2011) Body-weight–supported treadmill rehabilitation after stroke. N Engl J Med 364: 2026-2036.
[Crossref], [Google Scholar], [Indexed]
- Lura DJ, Venglar MC, van Duijn AJ, Csavina KR (2019) Body weight supported treadmill vs. overground gait training for acute stroke gait rehabilitation. Int J Rehabil Res 42: 270-274.
[Crossref], [Google Scholar], [Indexed]
- Miller EW, Quinn ME, Seddon PG (2002) Body weight support treadmill and overground ambulation training for two patients with chronic disability secondary to stroke. Phys Ther 82: 53-61.
[Crossref], [Google Scholar], [Indexed]
- Plummer P, Behrman AL, Duncan PW, Spigel P, Saracino D, et al. (2007) Effects of stroke severity and training duration on locomotor recovery after stroke: A pilot study. Neurorehabil Neural Repair 21: 137-151.
[Crossref], [Google Scholar], [Indexed]
- McCain KJ, Pollo FE, Baum BS, Coleman SC, Baker S, et al. (2008) Locomotor treadmill training with partial body-weight support before overground gait in adults with acute stroke: A pilot study. Arch Phys Med Rehabil 89: 684-691.
[Crossref], [Google Scholar], [Indexed]
- Atan T, Taskiran OO, Tokcaer AB, Karatas GK, Caliskan AK, et al. (2019) Effects of different percentages of body weight supported treadmill training in Parkinson‘s disease: A double-blind randomized controlled trial. Turk J Med Sci 49: 999-1007.
[Crossref], [Google Scholar], [Indexed]
- Lotfian M, Dadashi F, Rafieenazari Z, Shahroki A, Rasteh M, et al. (2019) The effects of anti-gravity treadmill training on gait characteristics in children with cerebral palsy. Annu Int Conf IEEE Eng Med Biol Soc 2019: 5256-5259.
[Crossref], [Google Scholar], [Indexed]
- Covarrubias-Escudero F, Rivera-Lillo G, Torres-Castro R, Varas-Díaz G (2019) Effects of body weight-support treadmill training on postural sway and gait independence in patients with chronic spinal cord injury. J Spinal Cord Med 42: 57-64.
[Crossref], [Google Scholar], [Indexed]
- Council of Europe (1997) Convention for protection of human rights and dignity of the human being with regard to the application of biology and biomedicine: Convention on human rights and biomedicine. Kennedy Inst Ethics J 7: 277-290.
[Crossref], [Google Scholar], [Indexed]
- Wu J, Wu B (2015) The novel quantitative technique for assessment of gait symmetry using advanced statistical learning algorithm. Biomed Res Int 2015: 528971.
[Crossref], [Google Scholar], [Indexed]
- Lee K, Kim ES, Jung B, Park SW, Ha IH (2021) Association between pain and gait instability in patients with lumbar disc herniation. J Int Med Res 49: 3000605211039386.
[Crossref], [Google Scholar], [Indexed]
- Kennedy RA, Carroll K, McGinley JL, Paterson KL (2020) Walking and weakness in children: A narrative review of gait and functional ambulation in paediatric neuromuscular disease. J Foot Ankle Res 13: 10.
[Crossref], [Google Scholar], [Indexed]
- Little VL, Perry LA, Mercado MWV, Kautz SA, Patten C (2020) Gait asymmetry pattern following stroke determines acute response to locomotor task. Gait posture 77: 300–307.
[Crossref], [Google Scholar], [Indexed]
- Rodríguez FJ, Valero-Cabré A, Navarro X (2004) Regeneration and functional recovery following peripheral nerve injury. Drug Discov Today Dis Models 1: 177-185.
[Crossref], [Google Scholar]


Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences